Latest findings: Therapy and religion can help those with unwanted same-sex attraction
by Christine Leow // September 9, 2021, 10:25 am

At a recent webinar, Dr Christopher Rosik shared yet-to-be published findings from his latest research about the efficacy of change-allowing therapies for those with unwanted same-sex attraction. Photo by Omar Elsharawy on Unsplash.
Talk therapy can help those who struggle with same-sex attraction (SSA) to pursue the change they want. However, religion and whether a person identifies as LGBT or not may play a significant part in that.
This was what emerged from Dr Christopher Rosik’s latest research that will soon be published.
The change in question is “generally viewed as occurring on a continuum” and something clients themselves want to pursue as a “self-determined goal”, he added.
“Change is never promised as an outcome of such therapies,” said the clinical psychologist and Director of Research at the Link Care Centre in California in the US.
The change in question is “generally viewed as occurring on a continuum” and something clients themselves want to pursue.
Dr Rosik is also a clinical faculty member of the Fresno Pacific University and has published more than 50 articles in peer-reviewed journals on dissociative disorders, homosexuality and other topics.
He was speaking on the topic Perceived Helpfulness of Change-Allowing Talk Therapy Among Clients with Unwanted Same-Sex Attraction as part of a series of webinars organised by Jason Wong.
Said Mr Wong: “This webinar is for parents and the public as well. I have met with a lot of parents who wanted to learn more about this, especially for those who know of someone – in their own family or home or have a friend – who struggle with sexual identity and same-sex attraction issues.
“I am doing this on my own personal, private capacity to help and support all of you who are helping and supporting others.”
Can we trust research on change-allowing therapies?
1. Why “conversion therapy” is a loaded term
Explaining his use of the term “change-allowing therapies”, Dr Rosik said that “conversion therapy” has become a “pejorative and deceptive term used by politicians and activists” more than anyone else and has “lost all its usefulness as a non-partisan” term.
He also challenged conventional wisdom that change-allowing therapies are harmful and ineffective, and that the science on the matter has been settled.

“Emerging research suggests at least two serious reasons for scepticism about these conclusions,” he said.
2. Research excluded non-LGBT+ identified people
Nearly all this literature samples LGBT+ identified people.
This is a problem because many, if not most, who experience SSA and pursue change-allowing therapies do not identify as LGBT+. In addition, most studies alleging harm recruit only LGBT+ identified people or exclude non-LGBT+ identified individuals.
“This may be analogous to determining the harms and benefits of marital therapy by only examining clients who have subsequently divorced to determine how effective or harmful marital therapy is,” said Dr Rosik.
3. Failure to control pre-therapy distress
None of the research controlled for pre-therapy levels of psychological distress and suicidality.
“This is a simple, basic research methodology 101. You must control for levels of the outcome variable present before the treatment is provided.”
“Far from increasing suicidality, recourse to SOCE generally reduced it.”
Research literature such as those by Assistant Professor of Social Work at the University of Southern California, John Blosnich (Blosnich et al, 2020), concluded that those exposed to Sexual Orientation Change Efforts (SOCE) were nearly twice as likely to have lifetime suicidal ideation.
However, the research did not factor in their degree of suicidality prior to SOCE. When that was taken into account, the results looked markedly different.
Research Associate Professor of Sociology at The Catholic University of America and priest Donald Sullins (Sullins, 2021) obtained the publicly available dataset from Blosnich. He identified an item measuring pre-SOCE suicidality ignored by Blosnich et al and reran Blosnich et al’s regressions adding this variable as a control.
This was what Sullins found: “After controlling for pre-existing conditions, there no longer remained any positive associations of SOCE with suicidality in the Generations data.
“Far from increasing suicidality, recourse to SOCE generally reduced it.”
The reduction of suicidality was not small. Following SOCE:
- Adults reduced suicide ideation by two-thirds
- Minors reduced suicide ideation by one-third
- Adults reduced suicide attempts by four-fifths
- Minors reduced suicide attempts by half
Heartening as the results were, Sullins felt the numbers may still “understate the beneficial effect of SOCE treatment on suicidality and affect”.
“Those who may have attained the goal of SOCE – to adopt heterosexual identity, orientation or sexual function – were systematically screened from the survey sample, which only included those currently identifying as a sexual minority,” he wrote.
Is change helpful or harmful?
Dr Rosik was recently involved in conducting new research that looked at change-allowing therapy with a more diverse sample pool.
As the only person on the six-person survey team who had not experienced SSA, he was invited to be part of the 4 Options Research to increase diversity of viewpoints.
Belief in the biological origin of SSA was, by far, the strongest variable in associating the psychotherapy goals as harmful.
“Such diversity is intended to increase critical thinking and limit confirmation bias, obtain a more diverse sample of SSA persons, and create accountability for how results are shared.”
The survey had over 200 questions in three sections and involved nearly 1,500 participants above the age of 18 “who had experienced SSA at some point in their life”.
The profile of the group included:
- Two-thirds men
- A little more than 40% identified as gay or lesbian, nearly 38% as heterosexual and slightly more than 13% as bisexual
- 1 in 5 had no religious affiliation while the rest were either Mormons, Christians or Catholics
- Nearly 10% indicated that they had “pursued one or more change related psychotherapy goal”
The first study of the survey – The Pursuit of Change and Acceptance of Same-Sex Attractions and Behavior in Psychotherapy – looked at whether participants perceived five psychotherapy goals, four of which were associated with change efforts, as having been harmful or helpful:
- Not to act on SSA
- Reduce SSA
- Eliminate SSA
- Feel heterosexual attractions (HSA)
- Affirm acceptance of SSA
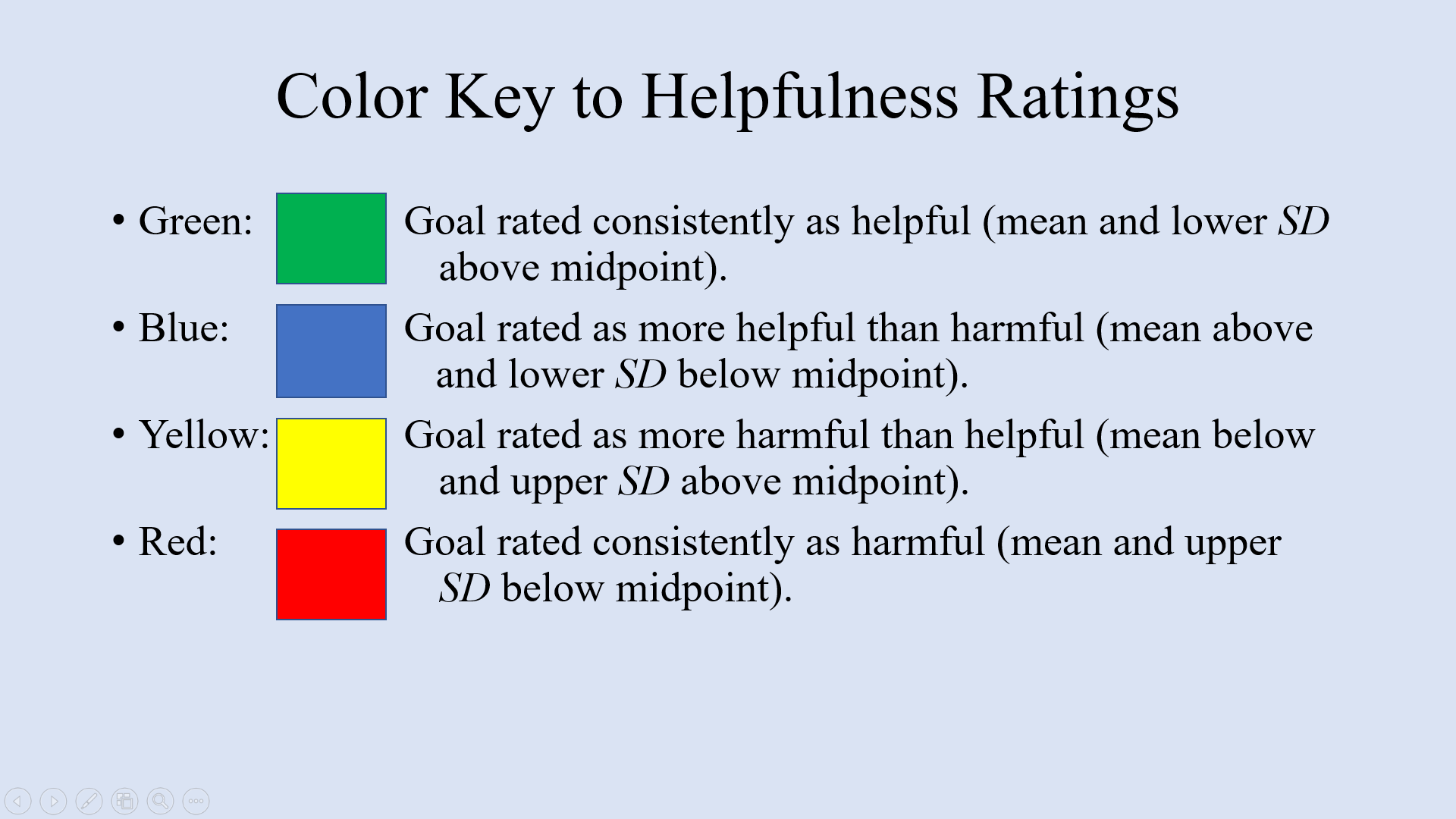
The survey asked participants to score the helpfulness or harmfulness of psychotherapy goals using these four measures. PowerPoint slide by Dr Christopher Rosik.
What the team found was that age, gender, race and education had no impact on whether people found the goals helpful or harmful.
“You really need research to have a much more nuanced understanding of who the participants are to understand who is being helped.”
Instead, religion played an important part in finding the psychotherapy goals helpful, as did not identifying as LGBT, despite having SSA. But those who believed that SSA was biological and not subject to change found the goals harmful. In fact, belief in the biological origin of SSA was, by far, the strongest variable in associating the psychotherapy goals as harmful.
So, for example, for the goal of not acting on SSA, those who were theologically conservative found the goal to be helpful, but those who did not identify as theologically conservative found the goal to be more harmful than helpful.
In the same way, those who experienced SSA but identified as non-LBGT found the goal helpful compared to those who identified as LBGT, who found it more harmful than helpful.
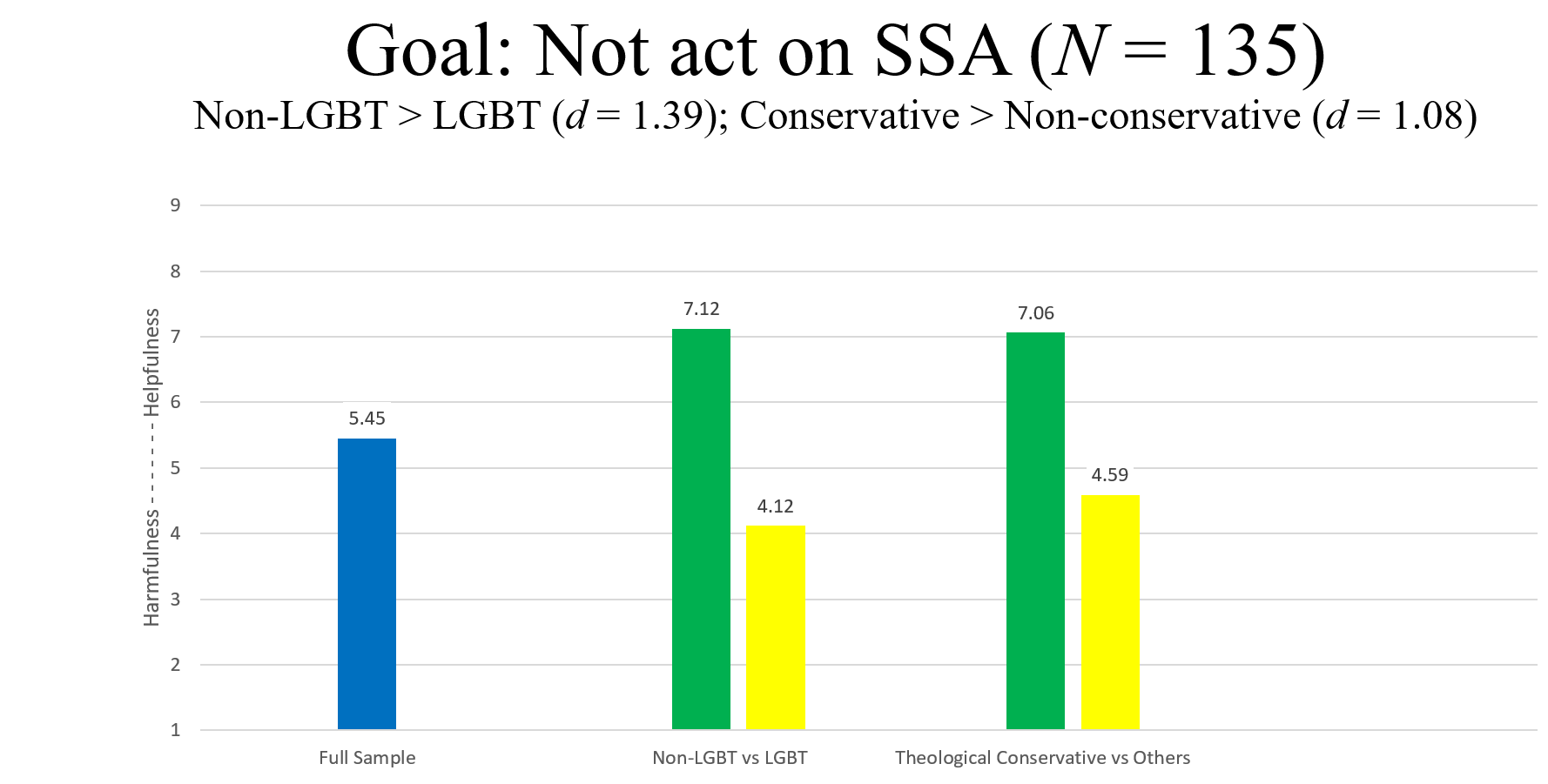
Though the Full Sample indicated that not acting on SSA was more helpful than harmful, it did not reflect the fact that those who identified as non-LGBT and theologically conservative found the goal helpful. PowerPoint slide by Dr Christopher Rosik.
“You really need research to have a much more nuanced understanding of who the participants are to understand who is being helped and who is potentially perceiving harm,” said Dr Rosik.
What the research revealed was illuminating:
- Reports of categorical sexual orientation change are fairly rare among clients presenting for psychotherapy.
- It cannot be known with certainty in advance who will experience help or harm from change-allowing therapy goals and, as such, caution is in order.
- Some highly religious and sexually fluid individuals appear to perceive their pursuit of change-oriented goals as helpful.
- Clinical work to accept one’s SSA (not necessarily identifying as LGBT+) appears reliably beneficial.
What helps those with unwanted SSA deal with their distress?
Of those surveyed, nearly 300 “indicated responding to their sexual orientation distress with one or more methods”.
In this second study of the survey, the profile of the group was:
- Mean age of about 40
- Two-third men
- Those with a religion – Mormons, Christians, Catholics, Jews – made up the majority
- Two-thirds had theological viewpoints (with 2 in 5 of them identifying as conservatives while the rest were not), the rest did not
- A little more than 60% identified as LGBT, the rest did not
Altogether 33 methods to address non-heterosexual sexual orientation distress were looked at and, again, participants were asked to rate them as helpful or harmful.
The preliminary findings of the research revealed several interesting points.
1. Neutral methods are helpful
Sexual orientation neutral methods were consistently perceived as helpful across the sample. These included:
- Identifying authentic needs and learning to meet them in healthy ways;
- Accepting sexual feelings without judgement and making decisions based on values;
- Learning strategies to reduce anxiety, depression, shame, and/or other mental distress;
- Learning assertiveness;
- Learning how to emotionally connect with others;
- Affirmation;
- Working through trauma;
- Helping others similarly distressed;
- Demystifying SSA.
2. Some methods usually thought to be helpful may not be
Some methods such as “coming out” may need to be contextualised to group-specific norms to be perceived as helpful.
This is because while the full sample registered this method as helpful, it did not reflect the fact that the theologically conservative found it only “more helpful than harmful” instead of entirely helpful as the full sample indicated.
Some methods often felt to be helpful – being naked but not sexual with same-sex others – remain clinically not advisable.
3. Aversive and punitive methods are harmful
Across the sample, aversive and punitive methods – anger, punishment and shame – were thought to be harmful.
4. Religion and sexual identity play a part
The helpfulness or harmfulness of many methods may be related to the client’s sexual identity label and theological perspective.
For example, for the method “Prioritizing my religious identity over my sexual identity”, although the overall sample showed it to be only slightly more helpful than harmful, the non-LGBT group found it to be helpful, but those with no theological leanings found it to be harmful.
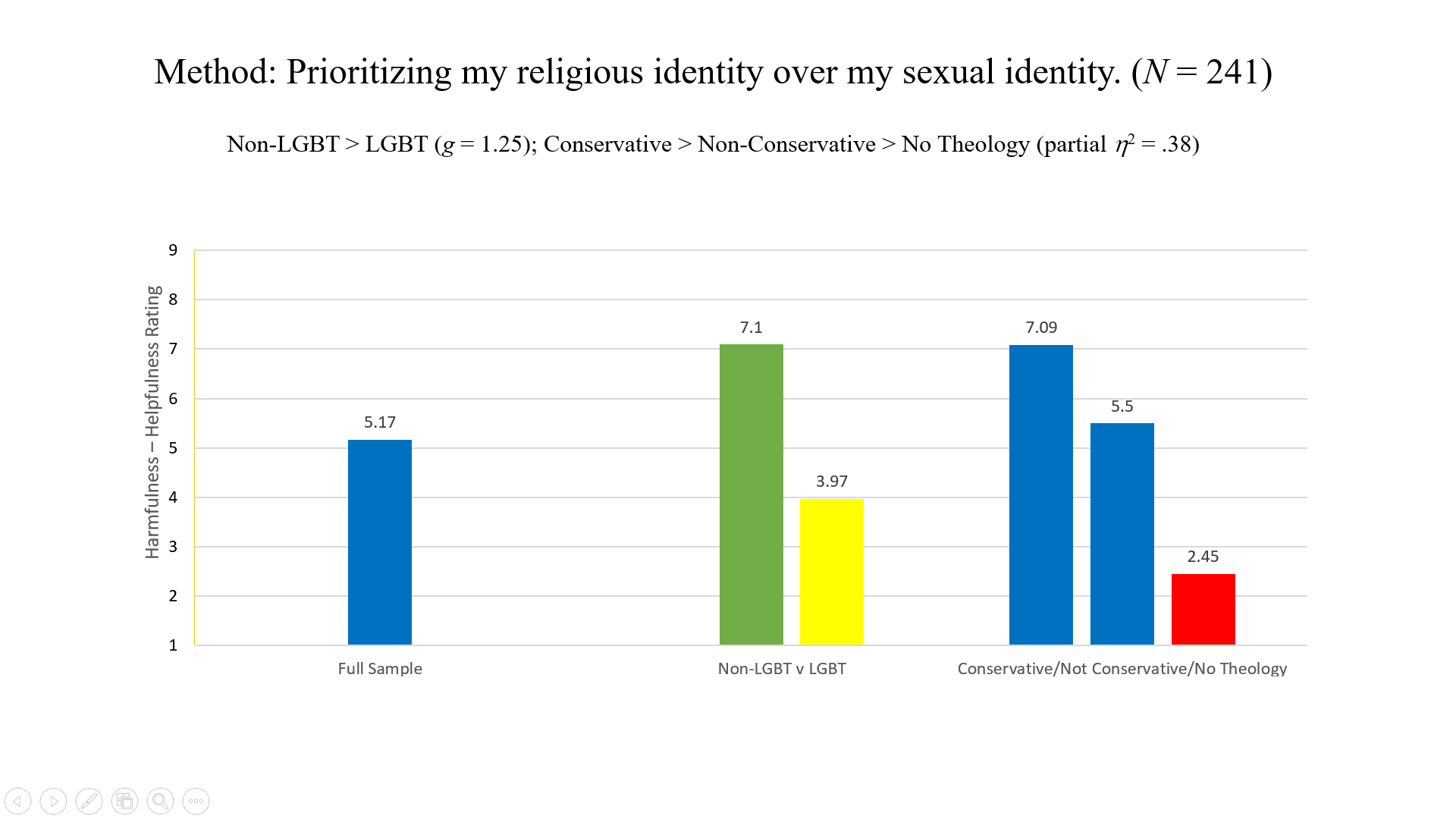
For this method of addressing non-heterosexual sexual orientation distress, the full sample, which indicated that the method was “more helpful than harmful” did not reflect the divergent assessment of those who identified as non-LGBT and those who did not have a theological perspective. PowerPoint slide by Dr Christopher Rosik.
In the same way, while the full sample found “Learning how others have reduced their same-sex attraction” only more helpful than harmful, the non-LGBT group found it helpful but those with no theological leanings found it harmful.
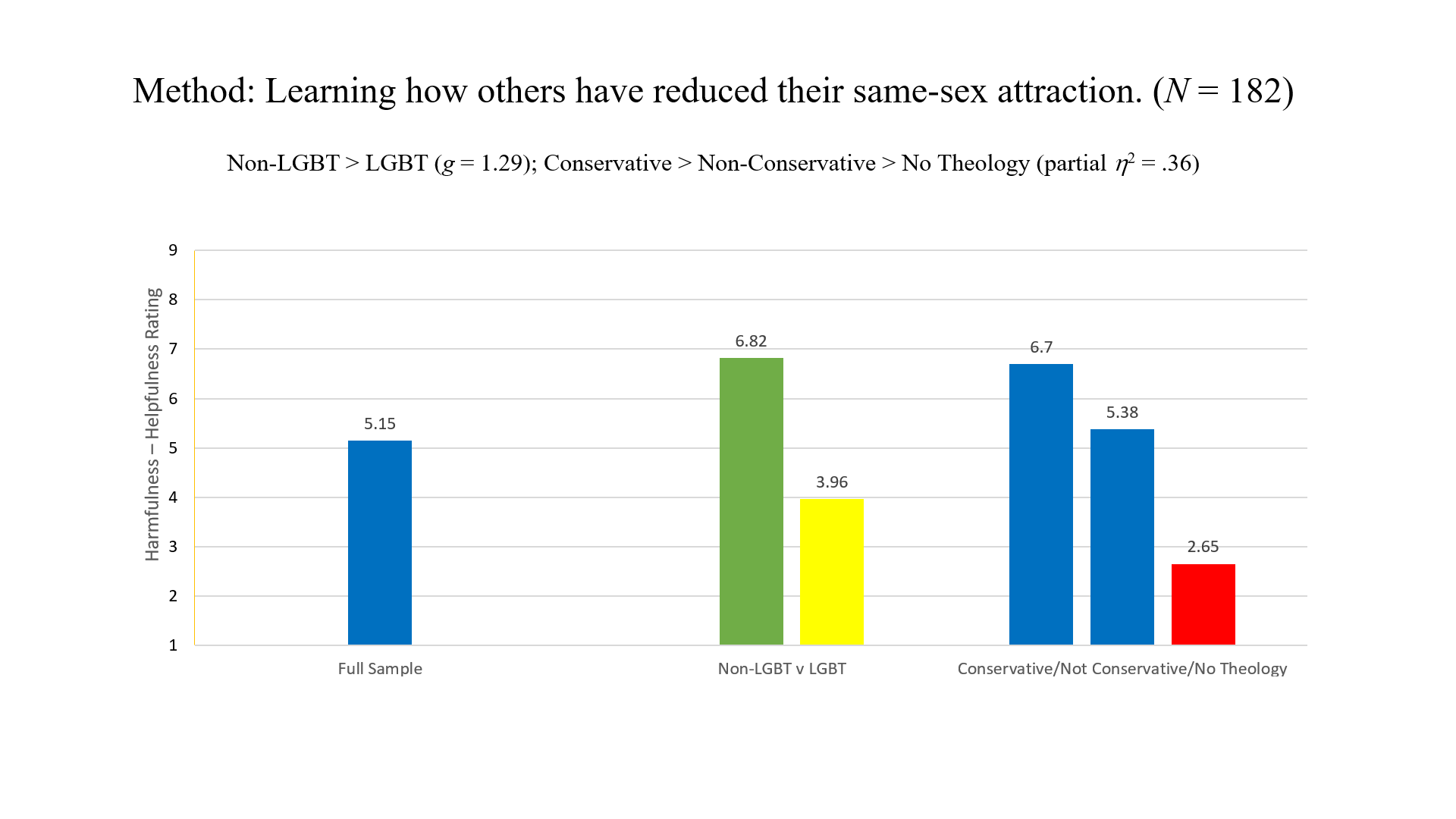
The full sample, once more, could not capture the differing scoring of the groups of participants. While the full sample indicated that the method was more helpful than harmful, those who identified as non-LGBT scored it as helpful and those with no theological perspective scored it as harmful. PowerPoint slide by Dr Christopher Rosik.
In fact, as the methods lean towards changing or reducing SSA and behaviours, those with no theological perspective scored them as harmful while those who identified as non-LGBT and conservative theologically favoured them.
“Lumping those coming from a conservative faith community … and those not in that community into one group is a disservice.”
The methods included:
- Intentionally not identifying as LGBT+ or adopting the label;
- Believing that homosexuality is a defence against the trauma of same-sex attachment loss that occurred in early childhood;
- Redirecting to HSA and enhancing these desires;
- Avoiding people and information that affirm LGBT+ issues;
- Resisting and trying to overcome sexual desires;
- Suppressing sexual fantasies and desires.
The researchers noted that “because helpfulness ratings of these methods evidenced greater variability in our sample and appeared to often vary by sexual identity labeling and theological perspective, we do not recommend that they be introduced to clients by the clinician”.
However, for those already engaging in such methods or want to use them, knowing “their attitude toward an LGBT+ identity label and their theological orientation can assist clinicians in providing guidance”.
Specifically, non-aversive methods that uphold a conservatively religious-based identity and promote restraint in SSA and behavioural enactments may provide modest benefit to many non-LGBT-identified individuals and/or individuals having conservative theological views.
5. Variations within the sample are telling
For many of the methods, the average full sample ratings were not reflective of the variations in the response of the different groups – LGBT, non-LGBT, theological conservatives, theological non-conservatives, no theological perspectives.
“When you get to the root, you see you need to know who you are looking at,” said Dr Rosik.
“Lumping those coming from a conservative faith community and how they want to address their SSA and those not in that community into one group is a disservice. And usually, the disservice is in the direction of those who are traditionally religious.”
How the research can be applied
Responding to the research, Raphael Zhang, one of the moderators of the Q&A segment of the webinar, said the affirmation that change-allowing therapies can help was heartening.
Sharing his personal journey, he said: “I believed I was born gay for the longest time.
“I pursued my gay desires because it feels, to a person with SSA, spontaneous, it feels natural, it feels like this doesn’t feel wrong, I can act upon it.
“I held the belief for 10-plus years.”
Then, he realised that his SSA may have come from “certain unmet needs in my childhood”. That caused a paradigm shift in his perspective.
“I had to revaluate for myself: Is it really true that everything I feel to be natural should be acted upon?”
“I started to see myself differently. It was empowering. Before, it felt like it was who I am, I can’t do anything about it.
“After that, I realised SSA is what I have and there is something I can do about this. There are decisions I can make.”
He added: “I always used to believe: If I feel it is natural, therefore it is right.
“After I went through that paradigm shift, I had to revaluate for myself: Is it really true that everything I feel to be natural should be acted upon? I have a lot of natural desires that I think should not be acted upon.
“It is authentic to live out who I am supposed to be versus being tied to my desires. It is more freeing to decide what desires you can act upon or not.”
Dr Rosik agreed, adding that what it means to be authentic is not what psychology can define.
“The belief that the experience I have must be my authentic self is a value judgement, not a scientific one,” he said.
Mr Zhang also raised the issue of “overgeneralisation of what change means”.
“People look at my story and say, ‘You haven’t really changed. You still have SSA.’ I feel like you should offer more space to let people define change in ways that are meaningful to them.
“I have SSA but am committed to not having same-sex behaviour and that, to me, is meaningful change. I think there should be space for that diversity of experience.”
Dr Rosik reiterated that shifts are considered change, too.
“This is the only area where the only kind of change that is considered to be helpful is a categorical one (that is, from having a homosexual orientation to a heterosexual orientation). That is a set-up.
“There is no other category of behaviour where that is the standard you have to meet for something to be considered helpful.”
What the research has indicated is that change is possible for those with unwanted SSA and that therapy can be a means of helping them towards that end.
RELATED STORIES:
https://saltandlight.sg/news/local-book-on-same-sex-attraction-among-christians-launched/
This year, as we celebrate 10 years, consider sowing into our Kingdom ministry! For S$10 a month, you become part of the #10for10 community and a part of every story we tell.
Partner with us
Related Articles

Are you a senior? Then it’s time to become a mountain-conqueror: Caleb Generation

One for Jesus: Church leaders gather to explore the changing face of evangelism

“When fathers arise, families flourish”: Elijah7000 rekindles fathering legacy of Dads for Life
